
The Punishment Equilibrium
How courts, jails, and housing providers get trapped in the safest deadly choice

People leaving jail or prison step into a statistical minefield, especially if they suffer from some sort of addiction. Overdose risk in the first weeks after release is many times higher than for the general population, yet the institutions that touch their lives keep doing the obviously bad thing—cutting off medications for opioid use disorder (MOUD), rationing diversion, and shunting people into unstable housing or the street. The puzzle we’re mulling over in this post is not “what should we value?” but something colder and more uncomfortable: how do our incentives make the worst outcomes the safest choice for the people who run the system?
The death trap, briefly
In my previous piece on this subject, I called this paradigm the quiet death trap: a world where everyone insists they are “following policy” while people with opioid use disorder (OUD) march through a predictable sequence—custody without medication, forced withdrawal, release into chaos, then overdose. We’ve known for years that continuing or initiating MOUD in custody sharply reduces post‑release overdose and often reduces reincarceration, but those practices are still the exception rather than the rule.
If you start from moral intuitions, nothing about this is mysterious. People who just survived jail or prison deserve a real chance not to die. If you start from institutional incentives, the pattern looks less like a tragedy of ignorance and more like an equilibrium—a grim balance where doing the right thing is punished and doing the deadly thing is quietly rewarded.
The players in the punishment game
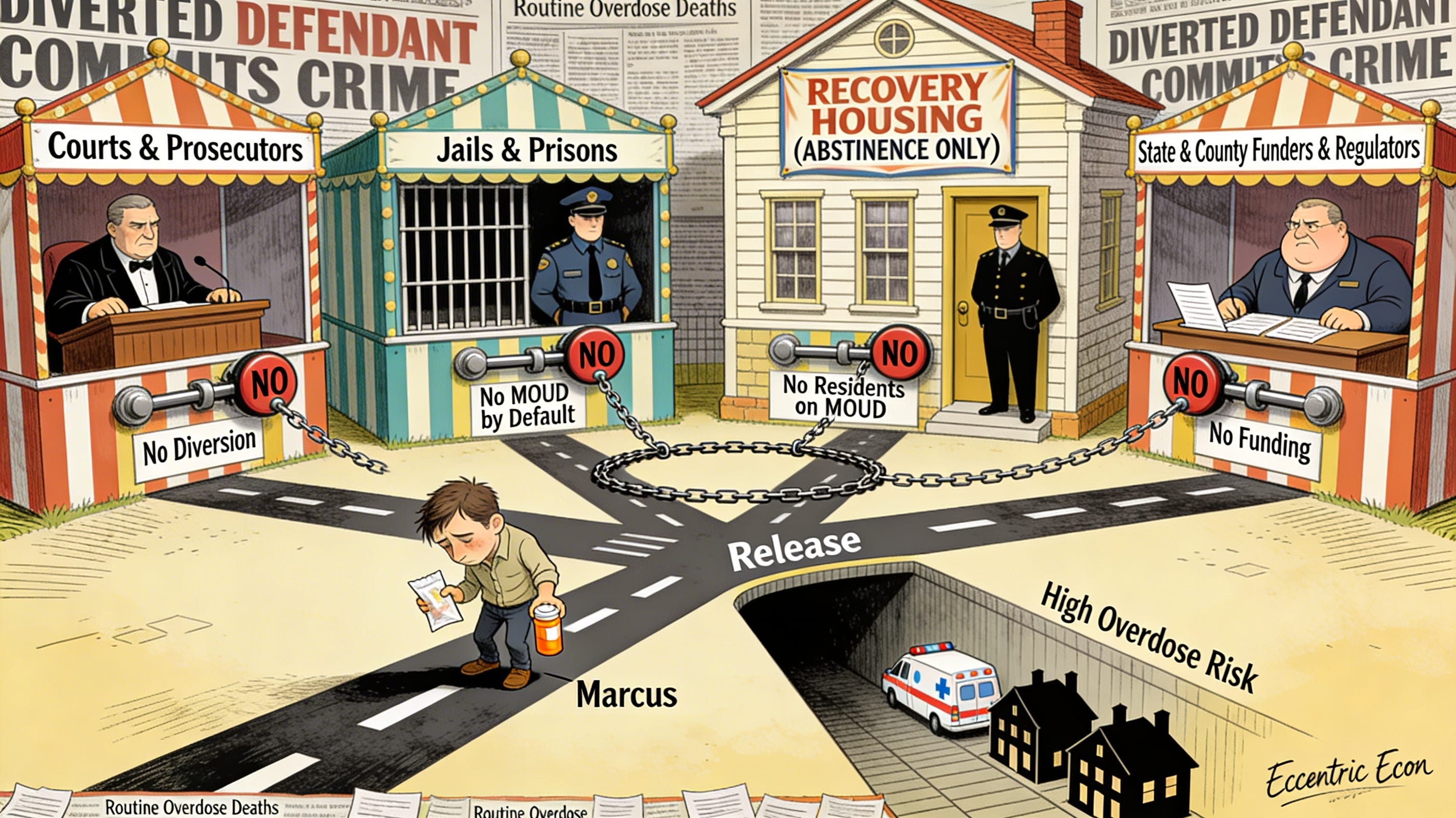
To see how that equilibrium forms, you don’t need a whiteboard full of equations, although I could certainly give you one. You just need to follow a small cast of characters and the pressures they face. Think of a typical person with OUD—let’s call him Marcus—moving through four sets of hands: courts and prosecutors, jails and prisons, recovery housing and treatment providers, and the state and county agencies that design the rules everyone else has to play by.
Each actor sees only a thin slice of Marcus’s life and only part of the harm. None of them wake up in the morning thinking “I want more people to die of overdose.” Yet each one faces intense, asymmetric pressure: they will be loudly blamed for some kinds of failure and barely noticed for others. Once you trace those asymmetries, “punishment as default” stops looking like a glitch and starts looking like the rational, if monstrous, outcome of the game they’re stuck in.
Courts and prosecutors: fear of the one bad story
Start with courts and prosecutors, who decide whether Marcus gets diverted to treatment or pushed through the standard criminal process. On paper, diversion looks like the humane and efficient choice: people with OUD get treatment instead of jail, the jail population falls, and future victimization may drop. In practice, the risk that dominates decision‑making is not the average outcome—it’s the nightmare headline.
If Marcus is diverted and later commits a high‑profile violent crime, the judge and prosecutor own that story. Their names are in the article, their faces in the news; op‑eds call them soft, legislators haul them into hearings. If Marcus is denied diversion, processed “by the book,” released after serving time without MOUD, and then quietly dies of an overdose in a motel room, that story barely exists as a story at all. The risk to Marcus is enormous; the risk to the court is effectively invisible.
So the sensible individual move is to underuse diversion. Say yes only when you’re certain, narrow eligibility, load programs with conditions that make it easy to terminate someone at the first sign of trouble. The rare visible crime weighs much more heavily in the internal calculus than the routine, invisible overdose after detention or harsh supervision. Over time, that bias toward avoiding the “one bad story” becomes standard practice.
Jails and prisons: paying for the wrong costs
Next, Marcus enters a jail or prison. Here the central question is simple: is MOUD the default, or is it an exception that requires special effort to access and maintain?
When MOUD is treated as optional or high‑friction, everything works against Marcus. Screening is perfunctory or inconsistent; people who were on methadone or buprenorphine in the community are tapered off or abruptly cut off upon entry; linkage to community care after release is spotty. Staff face operational costs—complex medication protocols, coordination with outside providers, diversion worries—without directly bearing the budgetary or political cost of what happens after someone walks out the gate.
From the correctional administrator’s perspective, MOUD is a line item: staff training, pharmacy contracts, secure storage, medication administration. Overdose deaths, emergency department visits, and future prison admissions show up in some other spreadsheet—hospital budgets, county coroners, state DOC population forecasts. In the payoff function the system implicitly writes, “cost of MOUD” is high and very salient, while “weight on post‑release overdose” is low and off‑stage. The predictable result is that custody without MOUD remains the default, even in jurisdictions that have formally authorized treatment.
Recovery housing: abstinence as a risk shield
Suppose Marcus survives release and looks for recovery housing or a residential treatment program. For someone with OUD, stable housing with some structure can be the difference between tenuous recovery and collapse. But here another set of incentives quietly pushes in the direction of exclusion.
Many housing providers operate under or internalize an abstinence‑only norm. They fear that allowing residents on methadone or buprenorphine will invite diversion, conflict with other residents, or trigger scrutiny from neighbors and funders. They directly experience any relapse or disruption that happens on their watch: a fight in the house, a positive urine screen, a neighbor complaint. They do not directly experience, or get measured on, the overdoses that occur after they discharge someone for medication use or for a minor rule violation.
So the safe move is to say no: no residents on MOUD, or only under cumbersome, stigmatizing conditions; quick termination for small violations; quiet pressure on people to taper off medications whether or not that’s clinically appropriate. The result is churn and instability—Marcus bounces between programs, couches, and shelters, each move eroding his fragile recovery while keeping each individual provider’s risk portfolio clean.
Funders and regulators: writing the rules of the game
Hovering above all of this are state and county funders and regulators. They don’t decide Marcus’s fate one case at a time; they write the scoring rules. They decide what gets reimbursed generously versus grudgingly, which performance metrics are tracked and rewarded, and how liability is assigned when something goes wrong.
When MOUD and supportive housing are under‑reimbursed, every jail administrator, treatment provider, and housing operator sees them as a private cost—a drain on their budget, their staff, their political capital. Overdose deaths and reincarceration, by contrast, are spread across budgets and agencies, or simply absorbed as background noise. Those outcomes may be expensive from a social perspective, but no single decision‑maker internalizes that cost. At the same time, media and political attention concentrate on visible failures: crimes by people who were diverted, housed, or kept on MOUD, not the deaths of those processed in the usual punitive way.
The upshot is a quiet but powerful message embedded in funding formulas and oversight: play it safe by saying no—no MOUD as default, no broad diversion, no MOUD‑inclusive housing networks.
What a punishment equilibrium looks like on the ground
Put those choices together and you get a “punishment equilibrium.” That’s just a fancy way of saying that each institution’s individually sensible move reinforces the others, so the whole system keeps snapping back to the same deadly pattern.
For Marcus, the path looks something like this: he’s arrested and, because a prosecutor worries about the one terrible headline, he’s denied diversion and held in jail. There, MOUD is not offered by default, or it’s made hard to access, so he goes through abrupt withdrawal in custody. When he’s released, his tolerance is low, his cravings are high, and his supervision conditions may be demanding and inflexible. He tries to get into housing, but providers either won’t accept him on medication or have already terminated him for a minor rule violation; he ends up in unstable housing or homeless.
Each of these decisions is locally defensible: the judge followed the risk assessment tool, the jail followed its medical protocol, the housing provider followed its abstinence policy. But taken together, they funnel most people with OUD through the highest‑risk corridor we know how to build—custody without MOUD, forced withdrawal, and unstable reentry—even though the system already has the capacity for a better path. That configuration, where punishment‑heavy choices are the default at each node, is what I mean by a punishment equilibrium.
Two quiet forces: money
The first force that holds this equilibrium in place is money, but not in the simplistic sense of “we don’t care enough to fund treatment.” It’s about who pays which costs and when.
In budget terms, MOUD programs and MOUD‑inclusive housing show up as explicit line items in the operating budgets of jails, prisons, and providers. They require hiring, training, and ongoing supervision. They may require physical changes to facilities and contracts with outside prescribers. By contrast, overdose deaths, emergency room visits, and reincarceration show up elsewhere—Medicaid claims, hospital uncompensated care, coroner reports, future prison bed projections.
When you under‑reimburse MOUD and supportive housing, you effectively turn them into a tax on the agencies that implement them. The social ledger might say “this is cheap, given the deaths and reincarceration avoided,” but the local ledger says “this is expensive and risky, and the savings go to someone else.” In the model language behind this series, the “cost of MOUD and housing” term in each actor’s payoff function is large and salient, while the weight they put on overdose outcomes is small. Under those conditions, the strategy profile where each actor under‑provides these services is not just possible; it’s stable.
Two quiet forces: blame
The second force is blame, which works like a kind of informal liability rule layered on top of the formal ones. Who gets blamed, and for what, shapes behavior at least as strongly as formal penalties.
Courts and housing providers are loudly blamed for visible failures—for the resident who commits a new crime while on diversion, for the person who overdoses in a house that allowed MOUD, for the parolee who makes the news. In legislative hearings and local news, those cases are read as evidence that someone was too lenient, too experimental, too willing to “take a chance.” The message to others is clear: if you stick your neck out, you may be uniquely punished for it.
Invisible failures look different. When someone dies of overdose after being processed “by the book”—denied diversion, cut off from medication in jail, discharged from abstinence‑only housing—there is rarely a hearing about that case, rarely an op‑ed about the judge who said no or the provider who enforced the abstinence rule. The family may grieve, advocates may take note, but the system does not treat those as institutional scandals.
Given that asymmetry, the individually safe move is to say no: no diversion, no MOUD as default, no MOUD‑taking residents. The more that “saying yes” concentrates visible risk on a few actors while spreading invisible harms across many, the more the punishment equilibrium becomes “stochastically stable”—in human language, the more it tends to re‑emerge after every shock, even if people sometimes try to move the system in a better direction.
The harm‑reduction equilibrium: a different path is possible
The bleakness of the punishment equilibrium might suggest that nothing else is feasible. But we have real‑world evidence that a very different regime is not only possible but effective. Call it a harm‑reduction equilibrium.
In this alternative configuration, diversion from jail to treatment is common and not treated as an exotic, special‑case tool. MOUD is the default in custody and at release—people come in on methadone or buprenorphine and stay on it, and those who meet clinical criteria can initiate in jail or prison. Recovery housing is explicitly MOUD‑inclusive by design, with structures and supports tailored to people on medication rather than against them. The cast of characters is the same, but the rules of the game differ: funding, metrics, and liability are aligned so that supporting treatment and stability is the safe move.
When Rhode Island implemented a comprehensive correctional MOUD program, it saw a large and clinically meaningful reduction in post‑incarceration overdose deaths and a measurable drop in overdose deaths at the state level overall. When Massachusetts mandated MOUD in county jails and expanded access in prisons, researchers documented higher post‑release MOUD engagement and lower risks of overdose, all‑cause mortality, and reincarceration among people who received treatment behind bars. The harm‑reduction equilibrium is not a utopian thought experiment; it is a configuration some places have already approximated.
Why better regimes don’t stick
If such a regime is feasible and better for nearly everyone, why doesn’t it spread and persist? Why isn’t Rhode Island’s model or Massachusetts’s jail reforms the new baseline everywhere?
Part of the answer is that in the current institutional environment, early adopters are exposed. The one generous judge who makes diversion the norm in her courtroom carries more headline risk than her colleagues while operating under the same blame rules. The one jail that makes MOUD the default shoulders higher up‑front costs, more operational complexity, and the risk that any future overdose involving a released participant will be pinned on that policy. The one housing network that leads on MOUD inclusion may find itself taking the highest‑needs residents, with little adjustment in reimbursement or regulatory support.
As long as the underlying money and blame structures remain unchanged, these first movers operate on a tilted playing field. They can improve outcomes in the short run, but they are constantly swimming against the current. Staff turnover, leadership changes, budget cuts, and political shocks—an election, a sensational crime, a budget crisis—each create an opportunity for the system to revert to the safer, more familiar configuration where saying no to people with OUD is rewarded and saying yes is punished. In the language of dynamic systems, the punishment equilibrium is the attractor: even if you push the system away from it, random disturbances and human error tend to pull it back.
Changing payoffs, not souls
If that story sounds fatalistic—if it makes you feel like the institutions are wired for punishment and always will be—that’s not where I want to leave you. The point of naming the punishment equilibrium is not to declare it inevitable; it’s to make clear where leverage really lies.
In the next post, I’ll turn to what it would mean to change the payoffs instead of changing the people: how modest shifts in funding, transparency, and default rules can make the harm‑reduction equilibrium the individually safe choice for judges, jail administrators, and housing providers rather than the risky one. That includes talking about the hard constraints that already exist: constitutional limits and disability‑rights law that quietly rule out some of the “cheap but deadly” strategies the system has leaned on for decades, like deliberate withdrawal of MOUD in custody or categorical exclusion of people on MOUD from publicly supported housing.
Those legal and institutional constraints are not a full solution, but they are part of a different game—one where Marcus’s survival is not a heroic exception but the ordinary result of ordinary decisions.